淋巴瘤可初步分為 B cell or T cell 或 Hodgkin Lymphoma (HL) or Non-Hodgkin Lymphoma (HL),又可依病程分為 indolent, aggressive, highly aggressive。
我們從 BCR/BTK signaling 在正常與惡性 B 細胞來看,可以得知 B cell survival 與 proliferation 中,BCR 啟動很重要,而 BTKi 會抑制其下游訊號。BTK 在 chemokine signaling 中,可以讓 B 細胞回到淋巴結,而 ibrutinib 的使用則會讓這些惡性細胞被趕出來到循環 (Wang, 2022; Hendriks, 2014)。
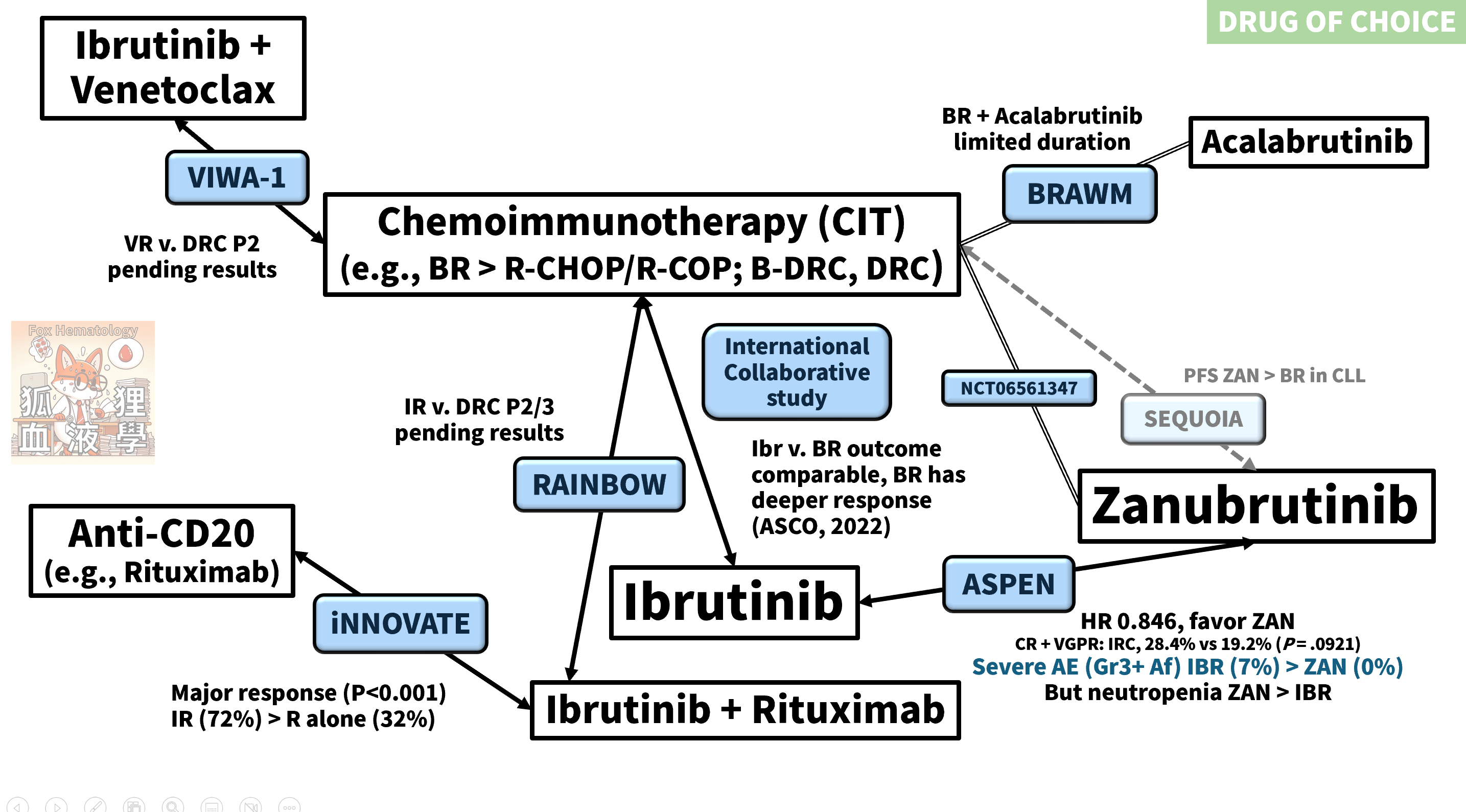
BTKi 在 B cell lymphoma 的試驗很多,知識更新的速度快,以下用表格整理一些比較重要的試驗。
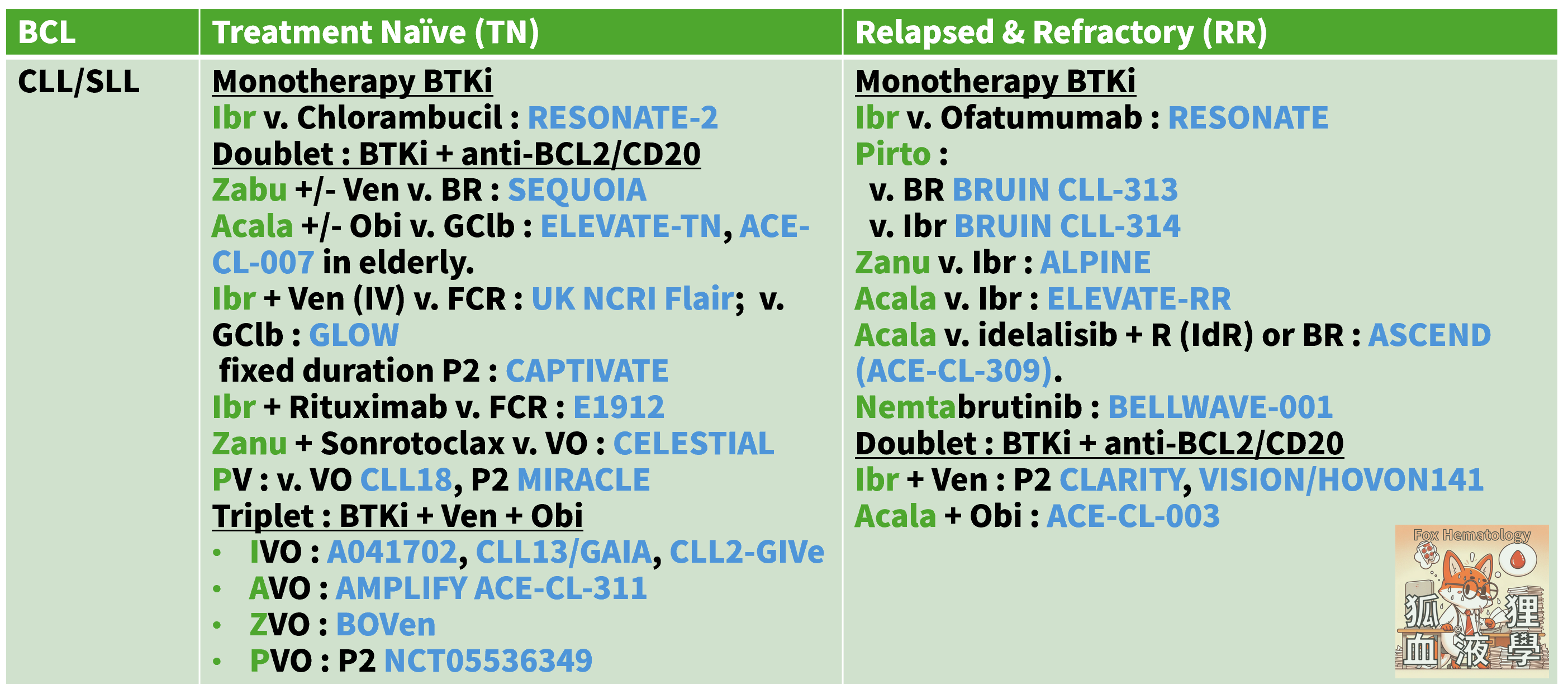
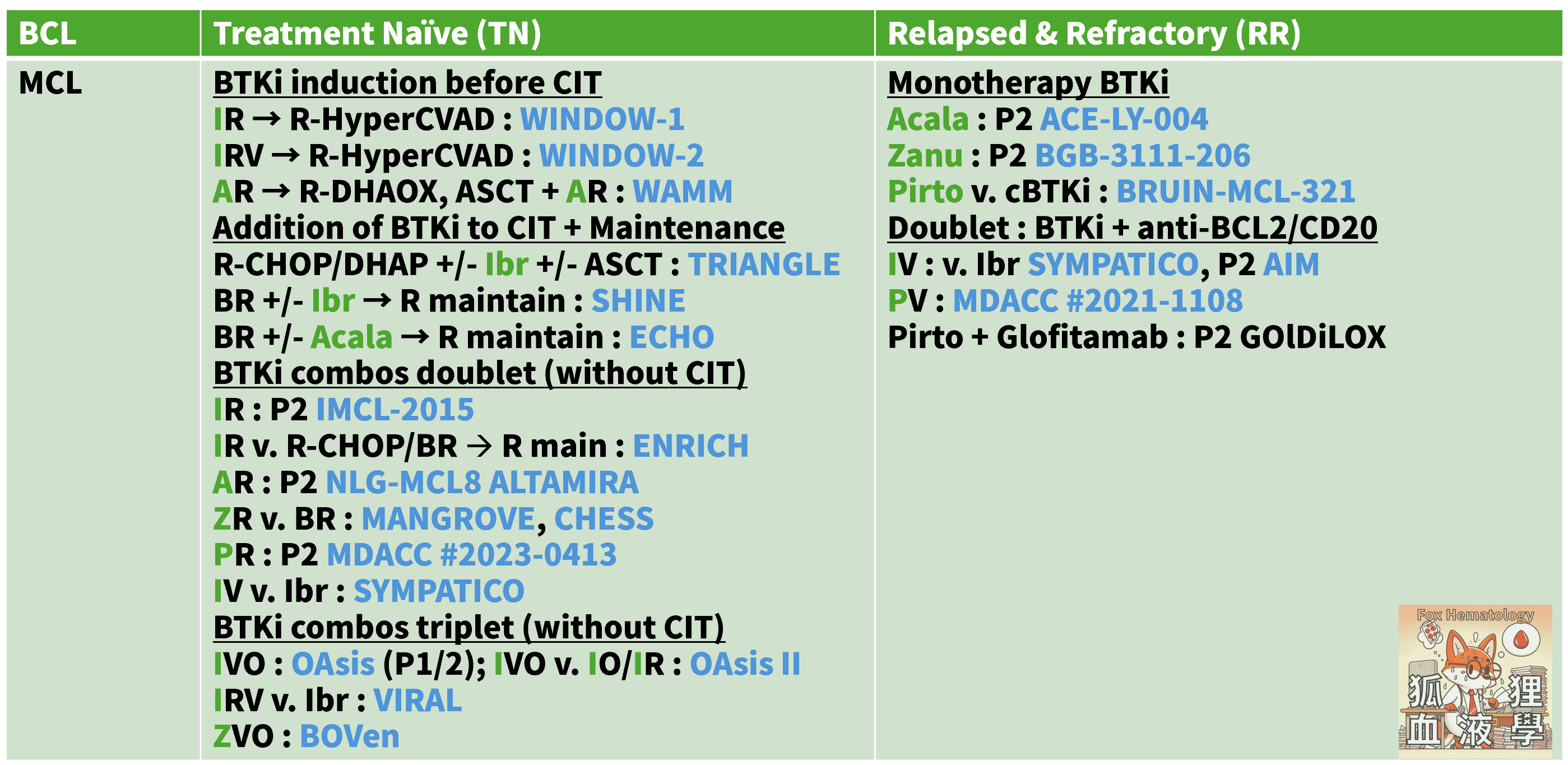
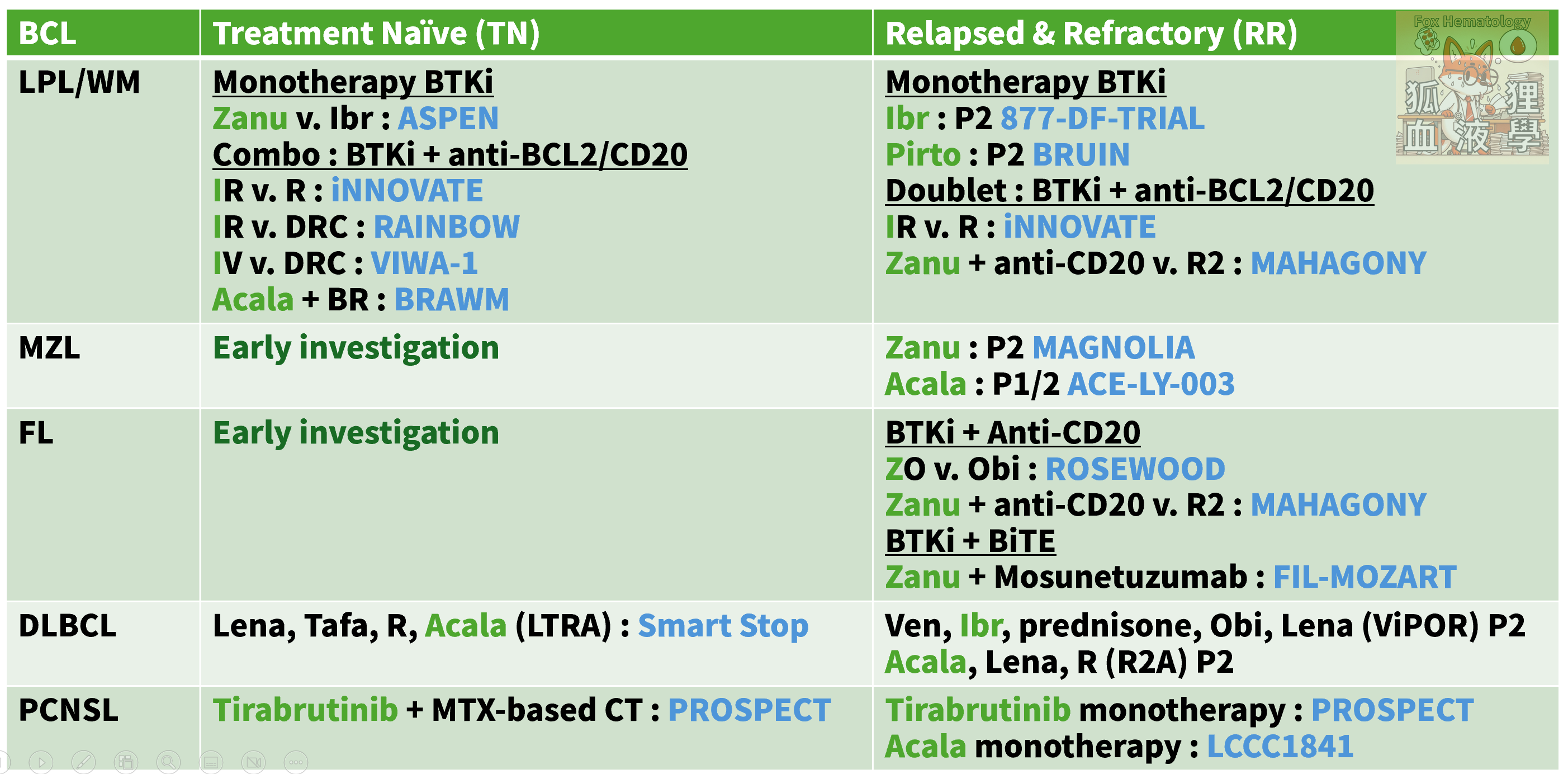
重點大至如下:
BTKi had activities across indolent B cell lymphomas even aggressive ones.
BTKi are mostly responsive in B cell lymphomas but need to be given continuously. Combining BTK inhibition with other agents might confer potential for limited-duration.
Different mutational profile in different B cell malignancies confer different response
BTKi selectivity influence spectrum of undesired targets & effects
Resistance to cBTKi might be overcome by use of non-covalent BTKi or even BTK degraders
Concentration in CSF of different BTKi suggests possible application in CNS diseases (e.g., PCNSL, SCNSL, Multiple sclerosis…).
今天和益欣學到了:(1) BTKi 第二代與第三代的心臟血管副作用有待更久的追蹤、(2) 高血壓藥物在 BTKi-induced hypertension 上要避免有 DDI 的 CYP3A4 代謝藥,包括 non-DHP (Diltiazam、Verapamil)、(3) BTKi 在小刀前停藥三天、大刀前後停七天、(4) BTKi induced hemorrhage 處置、(4) Afib 要盡早轉到心臟科進行 Rhythm control 以免 LA dilatation 太嚴重、(5) BTKi-induced HF 以 RAAS antagonist 治療為主。
試驗本身複雜,但臨床有更多要考量的。透過不同專科的視角,我們互相彌補短處,又各自發揮專長,吃頓好飯又能暢所欲言,樂哉。