


可量測殘存疾病 (Measurable Residual Disease, MRD) 在骨髓幹細胞移植的效用與誤用:摘錄評讀
本篇為 Othus, M., 等人 (2020). Statistics and measurable residual disease (MRD) testing: uses and abuses in hematopoietic cell transplantation 的摘錄評讀

原文為 Othus, M., Gale, R. P., Hourigan, C. S., & Walter, R. B. (2020). Statistics and measurable residual disease (MRD) testing: uses and abuses in hematopoietic cell transplantation. Bone marrow transplantation, 55(5), 843-850.
血癌病人是否要移植會基於三個面向來考量:(1) 病人本人、(2) 移植相關、(3) 疾病相關因子。而疾病相關因子有一大部份被 MRD 的結果所取代,亦即 MRD positive 會接受移植,negative 則可再觀察。
雖然 MRD 是個最好預測累積復發率 (cumulative incidence of relapse, CIR) 的指標,它的一致性統計量 (index of concordance, C-statistics) 只有 0.75。
C-statistics 在 Logistic regression 中即為ROC曲線 (Receiver operating characteristic curve, ROC curve) 下的區域 (Area under curve, AUC)。
MRD 的量測方式有許多種,不應該只用二元 (binary) 有/無的方式來判讀。
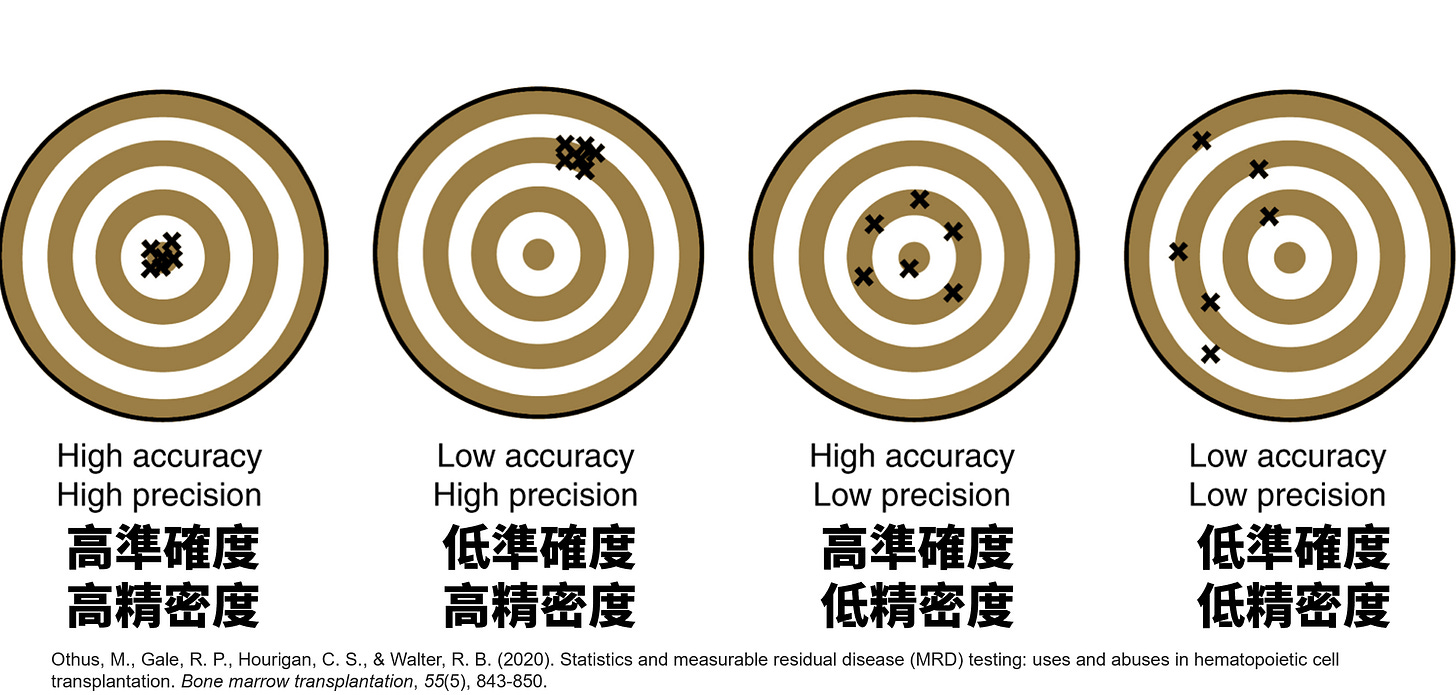
太過簡化的判讀方式忽略了這些檢驗的基本屬性、準確度與精密度,會犠牲統計檢定力 (statistical power, 或簡稱 power)、忽略組間差距(例:陽性但極低的 MRD 可能更接近 MRD negative 的病人,而不是 MRD 陽性且很大量的病人)。
純粹二元的分法會讓我們無法好好地建立 MRD 與預後的線性關係。至於非線性的關係,則可以考慮更多樣的方式,包括 Cubic splines 模式來分析 (link)。
「這個檢驗有多準」如何量化呈現?
許多研究想要找一個 MRD 的閾值 (threshold) 來進行二元劃分,反而預測表現上會更不佳。
MRD 研究的後續追蹤也十分重要。
有些試驗只追蹤兩年或五年,但 MRD 真正的意義還是在預測終生復發率。
可以用是否復發計算 MRD 的敏感性與特異性。

本文引用了兩段名言,都可以做為研究人的提醒:
Stephen Hawking : The greatest enemy of knowledge is not ignorance, it is the illusion of knowledge.
Voltaire : Doubt is not a pleasant condition, but certainty is an absurd one.



正在學習 flow cytometry 來做為 MRD 量測的過程中,與 qPCR 做 MRD 的經驗彼此交錯,在腦中踫撞。國外開會時問了學者一些問題,在此篇也得到方向。或許問題真正的答案不是肯定句,而是下一個問題。